How To Treat Achilles Tendinopathies
A tendinopathy is a degenerative disease of the tendon which can be a cause of severe pain and dysfunction. This article will discuss the treatment of tendinopathies specific to the Achilles Tendon.
- Introduction and Pathogenesis - What is a tendinopathy?
- Classification
- Treatment Approach for AT (insertional and mid-portion)
- Training Programme
- Conclusion
- Literature
1 Introduction and Pathogenesis - What is a tendinopathy?
Tendinopathies are common in sports and tendon problems in general are a highly prevalent orthopedic diagnosis, as they account for every third musculoskeletal consultation (Andarawis-Puri et al., 2015). The term tendinopathy is used to describe that both, inflammation and degeneration are present and responsible for the development of the condition (Abate et al., 2009). Initially, the term tendinitis was used to describe the nowadays known tendinopathy, because people believed it to be an acute inflammatory condition. But now we know that it's more of a degenerative condition (caused by too much or too little loading) in presence of some light inflammation markers. This means that putting on some ice and taking in anti-inflammatories will likely not make it better.
Tendinopaties can be very challenging to manage. The tie that binds all tendinopathies together is load. With Achilles and patellar tendinopathy being most present in the lower leg, other areas such as the flexor hallucis longus, tibialis posterior and tibialis anterior muscles are also affected by tendinopathies. They usually occur when the load put onto a tendon is greater than the tendons load capacity, that's why tendinopathies are very sport specific (or work specific) depending on which body part takes the most load.
Main takeaway: Tendinopathy is a loading related, degenerative condition,
There might exist a large inter-individual variability in tendon stiffness, causing some to develop a tendinopathy, while others don't. Excessively compliant tendons will be strained more for a given load and therefore degenerate faster than a stiff tendon.
But tendons, just like muscles, can adapt their structure to the demands placed upon them. As exercise will assist tendon healing through mechanotransduction and cause an up-regulation of insulin-like growth factor (IGF) which leads to better matrix remodelling (Sanchez Lbanez, 2015). Or as other authors put it: "Tenocytes, the main resident cells of the tendon, “sense” loads from the extracellular matrix (ECM), and in turn modulate the ECM. Loading therefore, is essential for the maintenance of tendon homeostasis, but can readily promote remodeling or degeneration" (Andarawis-Puri et al., 2015).
In the following we will focus on Achilles Tendinopathy (AT), which is the most prevalent condition of the Achilles tendon and is causing disability for athletes as well as people in the workplace.
Achilles tendinopathy is one of the most common lower limb tendinopathies and treating it is often challenging and can take anywhere between 3 and 12 months to fully recover. Active treatment approaches have shown to be superior to wait-and-see approaches in AT. In the long term (12 months) no differences were found between exercise, injection or combined treatments (van der Vlist et al., 2021) and therefore a calf exercising program is recommended for most people, as it is cost efficient, save and easy to perform.
Main takeaway: Due to the effects of exercise, it will make up the main treatment approach.
2 Classification of AT and Diagnosis
Classification:
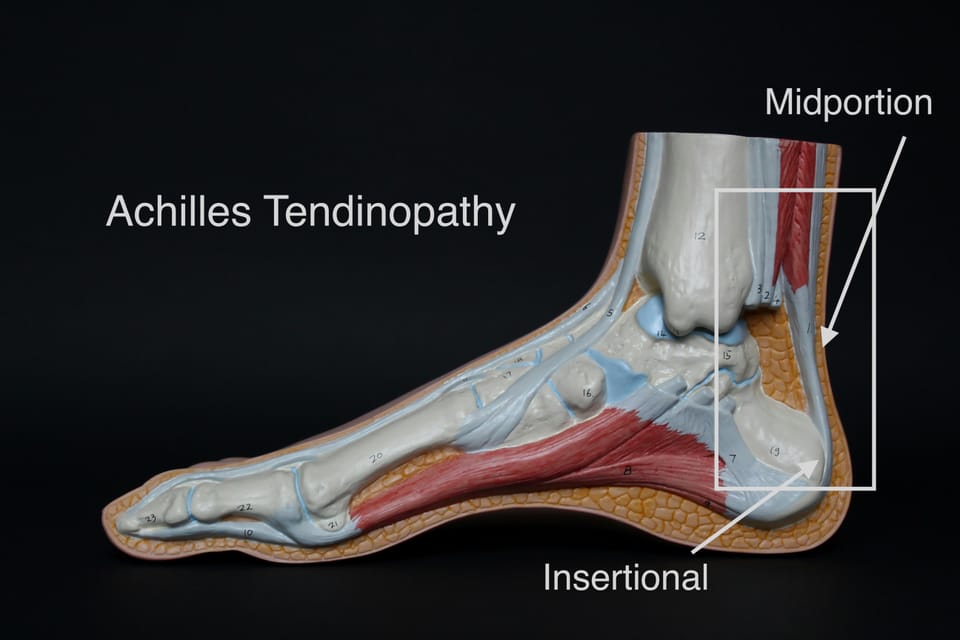
Achilles tendinopathy needs to be put into two different categories:
- Mid-portion AT
- Insertional AT
Mid-portion AT is the most common type, and being able to differentiate between the two types is critical when it comes to designing the treatment protocol.
Diagnosis:
The diagnosis can usually be made based on history and presentation.
In order to do so, you will want to identify load related pain, pain that is well localized at the Achilles tendon (mid-portion or insertion) and pain that gets better after warming-up and worse after the training in the patient. Typically people will present with an area of swelling and redness around the achilles tendon.
Simply palpating the tendon for pain is not a reliable way to assess for tendinopathy in active people, as an athletes tendons will almost always be sore to palpation.
A recent article nicely summarised known extrinsic risk factors to be "excessive mechanical overload and training errors such as increased interval training, abrupt changes in scheduling, excessive hill training, training on hard or sloping surfaces, increased mileage, increased repetitive loading, poor shock absorption, and wedging from uneven wear" (Ackermann et al., 2018).
Main takeaway: Look for recent increases in training load and pain that gets better after warming-up.
Differentiation:
Insertional AT will be painful around the tuber calcanei (= posterior aspect of the calcaneus), right at the insertion of the Achilles tendon. While mid-portion AT will be painful right around the middle of the Achilles tendon and is normally present around 2-6cm proximal to the calcaneal insertion (Singh et al., 2017).
Differential diagnosis:
In your differential diagnosis, check for: posterior impingement, tibialis posterior tendinopathy, referred pain of the lumbar spine. The differential diagnosis is an important part of treatment. It needs to be assessed to make sure no other condition can be responsible for the present symptoms.
3 Treatment Approach (insertional and mid-portion)
What the research says:
The management of tendinopathy cannot simply be a recipe-based exercise programme. As individual loading tolerance, previous sporting levels, future goals (concerning return to activity) and staging of the disorder needs to be taken into account. Exercise is the intervention with the highest level of evidence (Ackermann et al., 2018) for AT and will make up the main treatment appraoch. While exercise is the cornerstone of rehabilitating any tendinopathy, overloading the tendon too quickly can lead to further degeneration. Because when the overload exceeds the regenerative capacity of the tendon, the repair mechanisms are lost and the degeneration of the tendon begins. That said, the tendon needs to be subduced to external loading that is high enough to trigger some adaptation response, but it needs to be controlled. Slow- low impact resistance training and isometrics will make up the early stages of tendon rehab. Isometric exercises are used mainly for the analgesic effects and they should be performed as long as the patient is still hurting.
Rest will not get the tendon better, rather it will reduce the tendon loading capacity even further. Generally, we should try to reduce the loading on the tendon by reducing training load in the beginning, while correcting foot malalignments (if present) with orthotics and treat weakened muscles via exercises (Pearce & Tan, 2016).
In people with long-standing pathology, significant muscle atrophy will have occurred, which makes training the muscles attached to the tendon important, as it might have a sparing effect of the tendon, if the muscle can take up some of its work.
While some authors come to the conclusion that eccentric exercise programs are the superior exercise choice (Sivrika et al., 2023), others conclude that different training modalities (eccentric and heavy slow resistance training) elicit the same level of effectiveness (Beyer et al., 2015, Habets et al., 2017). We therefore recommend, that the training program chosen according to patient preference.
Indulging in an intensive 12-week exercise program has been shown to induce significant short- and long-term improvements regarding pain and function (Sivrika et al., 2023, Challoumas et al., 2023) and these results were sustained at the 1-year follow-up, when training was performed 3 times per week (Beyer et al., 2015). But to make sure the tendon has adapted properly, we recommend sticking to the training program for longer than that, even if symptoms might have faded at that point in time.
Exercises show improvement whether the pain sensation is felt of not. But patients will probably show better compliance if they can exercise pain-free while getting the same results (Kim et al., 2023).
Main takeaway: Sticking to some kind of a heel-raise centred training program for 12-weeks will likely lead to improved functioning in people with AT:
Psychological influences:
Before beginning to think about how to treat your particular client, think about "what’s the patients goal? what’s the starting point for this patient? which progression can we start with?". This will set you up for creating a patient-centred therapy approach.
In order to create an environment for optimal patient outcomes, in addition to a loading program, we need to include psychological and social factors into the treatment approach for it to be in alignment with the biopsychosocial model. A big part of that is pain education (especially important because chronic tendinopaties often go along with central sensitisation), where we need to make patients aware, that not all pain is harmful and that in tendinopathies, rehabilitation can include the perception of pain, which is acceptable and will not lead to further degeneration. As pain does not represent a direct correlation to tissue damage. This might help adress fear-avoidance or catastrophizing beliefs and lead patients to a more optimistic mindset. This is especially important in tendinopathies, as patients often fear that further damaging the tendon will lead to a rupture. This belief should be adressed by showing them that more harm will likely come from not sticking to an acitve loading program.
The next step is to educate patients about the treatment approach, why loading is more effective than rest in treating tendinopaties and how the patients are in control of their condition by adhering to the prescribed exercise protocol. We want to give patients a feeling of control and self-efficacy, which will likely produce better outcomes and make them more compliant (Edgar et al., 2022).
The Fear-avoidance Components Scale (FACS) can help determine the psychological state of individuals with tendinopathy (especially so with lower limb tendinopathies) (Neblett et al., 2016). To measure sport-injury-related fear avoidance, the Athlete Fear Avoidance Questionnaire (AFAQ) can be utilised to identify psychological barriers directed to the specific subpopulation of athletes (Dover & Amar, 2015), which are more likely to present with Achilles tendinopathy.
As in a recent qualitative study, patients beliefs about Achilles tendinopathy have been assessed and expressions like “I no longer feel like I'm in control of it now” arose during the interview. We need to make sure that we, as clinicians, coach people towards self-management through education, understanding and empowerment.
Main takeaway: Conduct a patient-centred therapy session and address any limiting beliefs your patients might have about his condition.
Exercise progression:
Transitioning from slow multi-joint movements to dynamic single-leg movements incrementally increases Achilles tendon loading. Seated heel raises loaded the Achilles tendon the least. This was explored in a recently (Baxter et al., 2021) and recommendations for progression were as such:
Begin with: Slow multijoint movements like squats, step ups and downs, lunges, walking, and double-leg standing heel raises applied similar loads to the Achilles tendon.
Increase to: Double-leg multijoint dynamic exercises like counter movement jumps, drop jumps, and hopping as well as running and single-leg standing heel raises.
End with: Single-leg movements like counter movement jumps, drop jumps, and hopping in different directions load the Achilles tendon the most.
From this study we can take, that for the most sensitive tendons, we can begin with the seated heel raise, then move up to single leg standing heel raises into double leg hops and finally single-leg forward hops, when looking for movements loading the Achilles. Looking at multi-joint movements, we could increase loads by starting with a squat into step downs and moving on with single-leg CMJ and then single-leg drop jumps.
Main takeaway: Seated calf raises form the earliest exercises for the most sensitive tendons and single-leg hops will wrap up the exercise program, as they have been shown to put the most strain onto the tendon.
4 Training Protocol:
The training protocol will be split up into 4 stages:
Stage 1: Isometrics
Stage 2: Heavy slow resistance training
Stage 3: Eccentrically focused strength training
Stage 4: Plyometrics
The increases in exercises and loading will be according to the progression model of the Silbenagel protocol: "Progression is made by changing from bipedal to unipedal exercises, by progressing from concentric-eccentric to purely eccentric loading, by adding weight in a backpack (in steps of 5 kg when pain did not exceed 5 on a 0–10 numerical rating scale), and finally by using fast-rebounding and plyometric exercises" (Habets et al., 2017). Exercising will be the most important part of rehabilitation: There needs to be increases in exercise load, frequency, endurance and speed throughout the rehabilitation process (Sivrika et al., 2023). Which is happening across the 4 stages.
Main takeaway: Increase exercises in load, progress from bipedal to unilateral and go from normal repetitions to heavy eccentric loading over time.
For insertional:
- Heel lift of a few cm is recommended (in order to reduce dorsiflexion in day to day movements and thereby minimise compression).
- Strengthen calf muscles without excessive dorsiflexion
- Typical symptoms are pain located at the insertion of the tendon and morning stiffness.
The biggest treatment difference for insertional and mid-portion tendinopathy is, that patients with insertional Achilles tendinopathy should avoid loading the tendon into dorsiflexion (which will increase compression and symptoms) and perform heel raises only to neutral in the earlier rehab stages while including additional services such as heel wedges (Chimenti et al., 2017). Roughly 1/3 of Achilles tendinopathies are insertional.
Good results have been shown when eccentric calf strengthening for 12-weeks was performed without loading the ankle in dorsiflexion in this population (Jonsson et al., 2008). Training like this will avoid any impinging between the tendon, bursa and bone.
- Exemplary protocol for insertional Achilles tendinopathy:
Stage 1: Start with double-legged isometric heel raises in weight bearing then add weight to that and eventually perform the isometrics single-legged.
Do: 5 sets of 45 second holds at approximately 70% MVC and 2 min break between sets
Stage 2: Start performing heel raised from the floor with both legs, then single legged. Perform the exercises both with straight knees (for gastrocnemius) and bent knees (for soleus).
Do: 3 sets of 15 each, and over time increase intensity while reducing repetitions.
Stage 3: Perform heel raises from the floor and focus on the eccentric phase (3 seconds eccentric), do that single legged and with extra weight. Perform the exercises both with straight knees and bent knees.
Do: 3-4 sets of 12 each, and increase volume over time.
Stage 4: Begin with plyometrics by adding hopping exercises (progress from bilateral to unilateral).
Do: 2 sets of 5 double legged forward hops and 2 sets of 5 unilateral CMJ.
For Mid-portion:
- Strengthen calf muscles anyhow
- Compression is not a problem here, so no adaptations need to be taken
- Typical symptoms: Pain located at the mid portion of the tendon and morning stiffness.
- Exemplary protocol for mid-section achilles tendinopathy:
Stage 1: Start with isometric heel raises in weight bearing then add weight to that and eventually perform the isometrics single-legged.
Do: 5 sets of 45 second holds at approximately 70% MVC and 2 min break between sets
Stage 2: Start performing heel raises from the floor with both legs, then single legged. Perform the exercises both with straight knees (for gastrocnemius) and bent knees (for soleus).
Do: 3 sets of 15 each, and over time increase intensity by reducing repetitions.
Stage 3: Perform heel raises from a step-up and focus on the eccentric phase (3 seconds eccentric), do that single legged with extra weight while lowering into deep dorsiflexion. Perform the exercises both with straight knees and bent knees.
Do: 3-4 sets of 12 each, and increase volume over time.
Stage 4: Begin hopping on the foot and forefoot.
Do: 2 sets of 5 double legged forward hops and 2 sets of 5 unilateral CMJ.
Tipps:
The time spent in each stage is not time, but function dependent. Meaning that if the patient in relatively quickly pain free and progresses to stage 2 and can perform single leg heel raises pain free and doesn't flare up the next day, he can safely progress to stage 3 and perform eccentric oriented exercises. Therefore, don't have someone perform the same exercises for weeks on end, and instead focus on their level of progression and how their tendon is reacting to the stimuli.
Stage 4 exercises are necessary for athletes only.
For pain regulation a numeric scale (3 out of 10) or traffic lights for pain: green (pain free) and yellow (light-moderate pain) and red (intense pain), can be used as an analogy to guide patients. They should stay green most of the time, while going into a bit of yellow is still okay (as it is in driving).
Additional recommendations:
When walking or running: barefoot loading (forefoot landing) should be avoided, as it puts more pressure on the soft tissues (loads the Achilles tendon more).
Heel wedges are recommended for insertional AT to decrease compressive loads (Cook & Purdam, 2012). Heel lifts can assists in reducing ankle dorsiflexion and are therefore a biomechanically sound adjunct treatment that can help reduce compression especially in people with insertional AT.
Soft tissue treatment (along the foot, ankle and calf) can be added to eccentric training (when done 2 times per week for 20-30 minutes) and has been shown to lead to slightly better improvements than only doing eccentric training regarding pain relief (McCormack et al., 2016). But in general, patients are educated and informed about their condition and manual therapy is only used as an adjunct to other evidence-based interventions.
According to a 2007 paper, performing an MRI can be a good predictor if surgery is needed. So imaging can be helpful in certain cases if conservative care fails (Nicholson et al., 2007).
5 Conclusion:
The presented training principles can be utilised for almost every tendinopathy. But making sure that the diagnosis is correct is the baseline for a good outcome. If after 4-6 weeks of consistent training no improvements in pain or function are seen, a different diagnosis should be considered.
This article has highlighted the importance of differentiating between mid-portion and insertional AT in designing treatment protocols. Exercise therapy has shown promising results in improving symptoms and function for patients with AT. Additionally, other modalities such as running technique and heel wedges may provide adjunctive benefits in pain management.
Moving forward, a comprehensive approach that considers individual patient goals and progression is crucial. Further research into the pathogenesis and treatment of AT is needed to enhance our understanding and improve outcomes for affected individuals. By implementing evidence-based interventions and individualised care plans, healthcare providers can effectively address the challenges posed by Achilles Tendinopathy and help patients regain optimal musculoskeletal health.
6 Literature:
Abate, M., Silbernagel, K. G., Siljeholm, C., Di Iorio, A., De Amicis, D., Salini, V., Werner, S., & Paganelli, R. (2009). Pathogenesis of tendinopathies: Inflammation or degeneration? Arthritis Research & Therapy, 11(3), 235. https://doi.org/10.1186/ar2723
Ackermann, P. W., Phisitkul, P., & Pearce, C. J. (2018). Achilles tendinopathy – pathophysiology: State of the art. Journal of ISAKOS, 3(5), 304–314. https://doi.org/10.1136/jisakos-2017-000164
Andarawis-Puri, N., Flatow, E. L., & Soslowsky, L. J. (2015). Tendon basic science: Development, repair, regeneration, and healing. Journal of Orthopaedic Research: Official Publication of the Orthopaedic Research Society, 33(6), 780–784. https://doi.org/10.1002/jor.22869
Baxter, J. R., Corrigan, P., Hullfish, T. J., O’Rourke, P., & Silbernagel, K. G. (2021). Exercise Progression to Incrementally Load the Achilles Tendon. Medicine and Science in Sports and Exercise, 53(1), 124–130. https://doi.org/10.1249/MSS.0000000000002459
Beyer, R., Kongsgaard, M., Hougs Kjær, B., Øhlenschlæger, T., Kjær, M., & Magnusson, S. P. (2015). Heavy Slow Resistance Versus Eccentric Training as Treatment for Achilles Tendinopathy: A Randomized Controlled Trial. The American Journal of Sports Medicine, 43(7), 1704–1711. https://doi.org/10.1177/0363546515584760
Challoumas, D., Crosbie, G., O’Neill, S., Pedret, C., & Millar, N. L. (2023). Effectiveness of Exercise Treatments with or without Adjuncts for Common Lower Limb Tendinopathies: A Living Systematic Review and Network Meta-analysis. Sports Medicine - Open, 9(1), 71. https://doi.org/10.1186/s40798-023-00616-1
Chimenti, R. L., Bucklin, M., Kelly, M., Ketz, J., Flemister, A. S., Richards, M. S., & Buckley, M. R. (2017). Insertional achilles tendinopathy associated with altered transverse compressive and axial tensile strain during ankle dorsiflexion. Journal of Orthopaedic Research: Official Publication of the Orthopaedic Research Society, 35(4), 910–915. https://doi.org/10.1002/jor.23338
Cook, J. L., & Purdam, C. (2012). Is compressive load a factor in the development of tendinopathy? British Journal of Sports Medicine, 46(3), 163–168. https://doi.org/10.1136/bjsports-2011-090414
Dover, G., & Amar, V. (2015). Development and Validation of the Athlete Fear Avoidance Questionnaire. Journal of Athletic Training, 50(6), 634–642. https://doi.org/10.4085/1062-6050-49.3.75
Edgar, N., Clifford, C., O’Neill, S., Pedret, C., Kirwan, P., & Millar, N. L. (2022). Biopsychosocial approach to tendinopathy. BMJ Open Sport & Exercise Medicine, 8(3), e001326. https://doi.org/10.1136/bmjsem-2022-001326
Habets, B., van Cingel, R. E. H., Backx, F. J. G., & Huisstede, B. M. A. (2017). Alfredson versus Silbernagel exercise therapy in chronic midportion Achilles tendinopathy: Study protocol for a randomized controlled trial. BMC Musculoskeletal Disorders, 18(1), 296. https://doi.org/10.1186/s12891-017-1656-4
Jonsson, P., Alfredson, H., Sunding, K., Fahlstrom, M., & Cook, J. (2008). New regimen for eccentric calf-muscle training in patients with chronic insertional Achilles tendinopathy: Results of a pilot study. British Journal of Sports Medicine, 42(9), 746–749. https://doi.org/10.1136/bjsm.2007.039545
Kim, M., Lin, C.-I., Henschke, J., Quarmby, A., Engel, T., & Cassel, M. (2023). Effects of exercise treatment on functional outcome parameters in mid-portion achilles tendinopathy: A systematic review. Frontiers in Sports and Active Living, 5, 1144484. https://doi.org/10.3389/fspor.2023.1144484
McCormack, J. R., Underwood, F. B., Slaven, E. J., & Cappaert, T. A. (2016). Eccentric Exercise Versus Eccentric Exercise and Soft Tissue Treatment (Astym) in the Management of Insertional Achilles Tendinopathy. Sports Health, 8(3), 230–237. https://doi.org/10.1177/1941738116631498
Neblett, R., Mayer, T. G., Hartzell, M. M., Williams, M. J., & Gatchel, R. J. (2016). The Fear-avoidance Components Scale (FACS): Development and Psychometric Evaluation of a New Measure of Pain-related Fear Avoidance. Pain Practice: The Official Journal of World Institute of Pain, 16(4), 435–450. https://doi.org/10.1111/papr.12333
Nicholson, C. W., Berlet, G. C., & Lee, T. H. (2007). Prediction of the success of nonoperative treatment of insertional Achilles tendinosis based on MRI. Foot & Ankle International, 28(4), 472–477. https://doi.org/10.3113/FAI.2007.0472
Pearce, C. J., & Tan, A. (2016). Non-insertional Achilles tendinopathy. EFORT Open Reviews, 1(11), 383–390. https://doi.org/10.1302/2058-5241.1.160024
Sanchez Lbanez, J. M. (2015). New Treatments for Degenerative Tendinopathy, focused on the Region-Specific of the Tendon. Rheumatology: Current Research, 05(04). https://doi.org/10.4172/2161-1149.1000173
Singh, A., Calafi, A., Diefenbach, C., Kreulen, C., & Giza, E. (2017). Noninsertional Tendinopathy of the Achilles. Foot and Ankle Clinics, 22(4), 745–760. https://doi.org/10.1016/j.fcl.2017.07.006
Sivrika, A. P., Papadamou, E., Kypraios, G., Lamnisos, D., Georgoudis, G., & Stasinopoulos, D. (2023). Comparability of the Effectiveness of Different Types of Exercise in the Treatment of Achilles Tendinopathy: A Systematic Review. Healthcare (Basel, Switzerland), 11(16), 2268. https://doi.org/10.3390/healthcare11162268
van der Vlist, A. C., Winters, M., Weir, A., Ardern, C. L., Welton, N. J., Caldwell, D. M., Verhaar, J. A. N., & de Vos, R.-J. (2021). Which treatment is most effective for patients with Achilles tendinopathy? A living systematic review with network meta-analysis of 29 randomised controlled trials. British Journal of Sports Medicine, 55(5), 249–256. https://doi.org/10.1136/bjsports-2019-101872
Vieira, C. P., Guerra, F. D. R., de Oliveira, L. P., Almeida, M. S., Marcondes, M. C. C., & Pimentell, E. R. (2015). Green tea and glycine aid in the recovery of tendinitis of the Achilles tendon of rats. Connective Tissue Research, 56(1), 50–58. https://doi.org/10.3109/03008207.2014.983270